The internet has become an integral part of our lives, offering both connection and entertainment. Ákos Arató (Hungarian Academy of Sciences, 2024) points out, however, that deepening reliance on tech has led to concerning behavioral addictions, prompting research into their psychological impacts.
* * *
The ubiquitous and growing use of the internet, along with other digital tools, has brought about radical changes in society, making online devices an indispensable part of our lives. Over the past decade, in particular, the internet has gained a more prominent place in many areas of our lives as a fast and easy way of connecting with others, as a source of entertainment, and as a provider of instant answers to the challenges of everyday life. With smartphones now in everyone’s pocket, people can access a wealth of content that gives us positive feedback and offers respite from the difficulties of everyday life.
At the same time, the high functionality of the internet can, depending on personal disposition, easily lead to disorders similar to behavioral and substance addictions, such as problematic internet use (PIU) (Young, 1998), problematic smartphone use (Panova & Carbonell, 2018), and problematic social media use (Hou et al., 2019).
Nearly 68% of the world’s population uses the internet on a daily basis; in many European countries, this figure exceeds 90% (Iceland 100%, Norway 98%, Denmark 96%, United Kingdom 95%, Germany 94%). In Asia, almost 97% of the population in South Korea has access to the internet, while the figure in China is nearly 70%. The fastest growth in internet use over the last decade, though, has been in the developing countries of Africa (Mali 60%, Cameroon 33%) (World Stats, 2023).
As for mobile devices, nearly 80% of people around the world have a device that enables them to stay connected online, and more than 50% believe that access to the internet is an essential part of their daily lives (Fuchs et al., 2018). It is currently estimated that 6% of the world’s population is affected by PIU (Hull & Proulx, 2022), which suggests that these disorders are considered a new and relatively fast-growing mental health concern.
In the light of the prevalence of digital devices and the growth in disorders related to their use, I have chosen to focus my research on internet use, and more specifically, the impact of PIU on psychological well-being, psychological functioning, and underlying neurobehavioral functions.

Some people have compulsive thoughts about their internet-related activities.
Psychological Consequences of PIU
PIU is frequently defined as a form of behavioral addiction (Brand et al., 2016). PIU includes the uncontrolled use of the internet, obsessive thinking about it, or the neglect of other activities, such as daily chores, work, and social life (Demetrovics et al., 2008). All addictions have both psychological and physical characteristics, and PIU is no exception. The physical symptoms occur mostly during the withdrawal phase, while the psychological symptoms, such as anxiety, appear in the absence of the object of the behavioral disorder.
As a behavioral addiction, PIU is best understood through psychological symptoms, such as depression, anxiety, interpersonal problems, sleep deprivation, compulsive behaviors, low self-esteem, and emotional distress (Mihajlov & Vejmelka, 2017). When problematic users are prevented from engaging in their addictive activities for any reason, they experience various emotional withdrawal symptoms. More impulsive, aggressive, and compulsive behavioral reactions are also not uncommon (Park et al., 2014). This is not surprising, as withdrawal symptoms are generally accompanied by low self-control.
In addition, many researchers have found that problematic users are unable to regulate their emotional reactions (Caplan, 2010), which not only results in poor emotion regulation strategies but also affects their ability to cope with behavioral difficulties. Behavioral disorders like PIU can thus easily develop in the absence of adequate self-control and emotional regulation (Brand et al., 2016).
In terms of psychological disorders, it is generally agreed that there is a positive relationship between depressive symptom levels and internet use (Andreassen et al., 2016) and a negative relationship between heavy use of social networking sites and self-esteem (Malik & Khan, 2015). Heavy internet use can have negative consequences for individuals’ personality and social life (Griffiths, 2014) and can also lead to difficulties in work and academic performance.
However, it is important to note that the direction of the relationship between social media and various psychological outcomes is often unclear. It is possible that an individual’s depressive and anxious nature contributes to spending more time on social networking sites, while the reverse can also be true (L. Y. Lin et al., 2016). The fact that individuals’ prior psychological distress can be considered a risk factor for PIU may provide some explanation for this dichotomy. Of course, problematic internet and social media use may also increase the level of prior distress and contribute to the likelihood of depression onset (Gámez-Guadix et al., 2015).
Brand’s Model on the Development and Maintence of Internet-Use Disorders
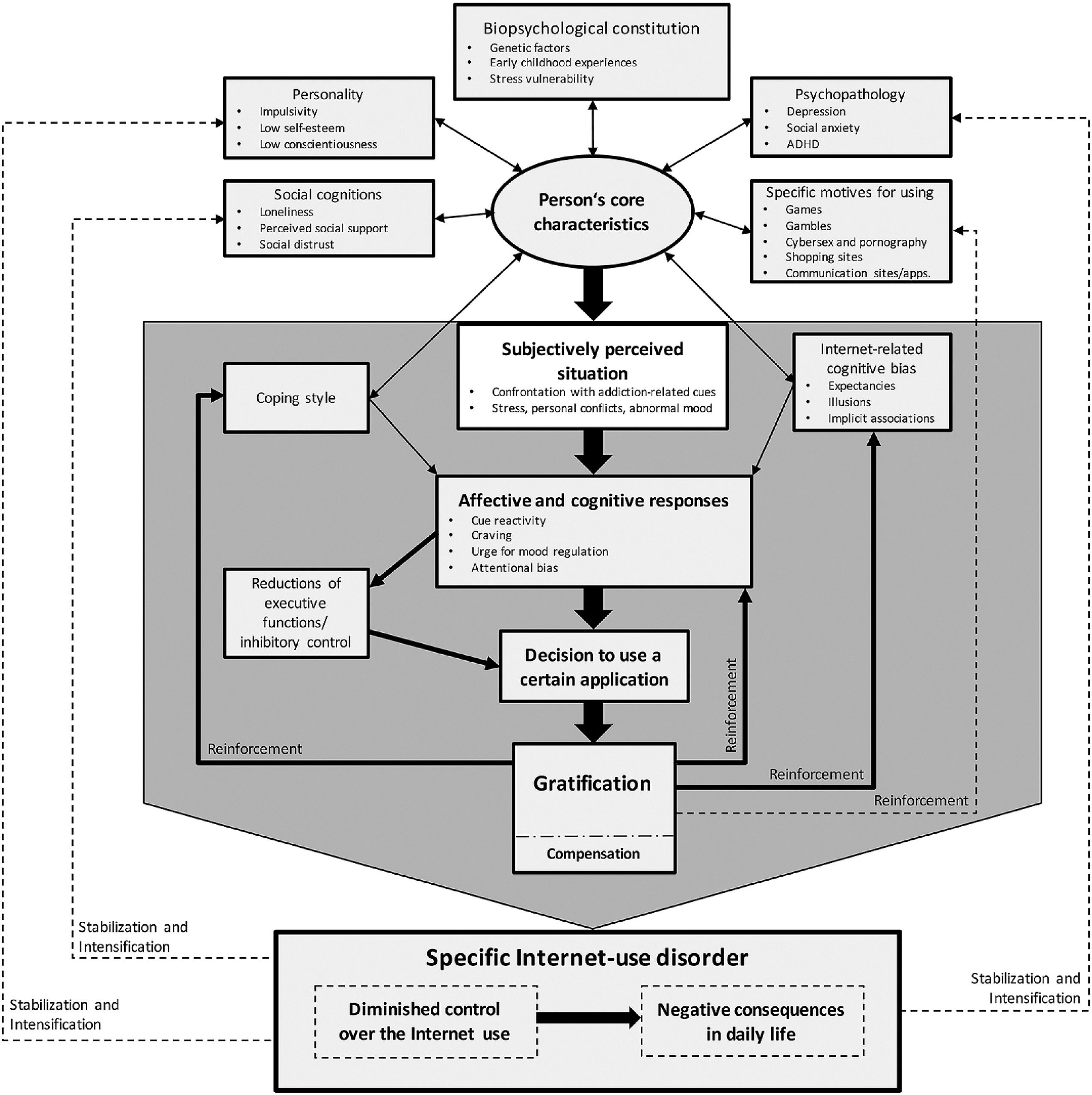
Note: Bold arrows represent the main pathways of the addiction process.
Functional Brain Alterations and Future Directions in PIU
Several studies, moreover, have been conducted to investigate the effects of PIU on various cognitive functions (Weinstein, 2022). These studies have mainly used functional and structural magnetic resonance imaging to investigate the underlying neural alterations behind cognitive functions in PIU.
These studies found structural and functional alterations in the brain’s reward (Altbäcker et al., 2016), executive (Darnai et al., 2019), inhibitory control (Dong et al., 2012), language (Darnai et al., 2022), social (Arató et al., 2023), and default mode (Darnai et al., 2019) systems, which were associated with reduced cognitive and executive control, diminished attentional processes, and impaired emotion regulation.
Altered functioning of executive and cognitive control functions are prerequisites for the development and maintenance of addictive disorders (Brand et al., 2016). And a decline in cognitive control functions and emotional regulation is a common phenomenon across different addictions.
Given these higher-level brain alterations, I believe it is important to explore what other higher-order functions might be associated with PIU. Therefore, for many years, the main theme of my research has been to investigate different psychological states and their possible neurological underpinnings in young adults with PIU.
Previous studies in which I have been engaged have confirmed the altered functioning of inhibitory and default systems in the brain (Darnai et al., 2019). And we have shown for the first time that social cognitive functions (the recognition of emotional facial expressions) and the underlying neural functions are associated with PIU levels in young adults (Arató et al., 2023).
In my present study, I am investigating mental fatigue in individuals with PIU. Long-term fatigue is a common symptom in addictions and is often reported by those diagnosed with PIU (Bachleda & Darhiri, 2018). The extent of PIU, moreover, has an independent effect on the level of perceived long-term mental fatigue (S. C. Lin et al., 2013). Spending a lot of time online and being constantly fed internet-related cues may lead to permanent fatigue in daily and professional life and could result in higher safety risks (Nachreiner, 2001), occupational issues (Williamson et al., 2011), and traffic accidents (Zeller et al., 2020).
Due to the lack of studies in this area, I would like to fill the gap in the scientific literature and provide a scientifically based foundation for appropriate preventive and therapeutic methods to reduce the amount of long-term and task-induced fatigue caused by PIU and thereby increase the psychological well-being of individuals.
References
Altbäcker, A., Plózer, E., Darnai, G., Perlaki, G., Horváth, R., Orsi, G., Nagy, S. A., Bogner, P., Schwarcz, A., Kovács, N., Komoly, S., Clemens, Z., & Janszky, J. (2016). Problematic internet use is associated with structural alterations in the brain reward system in females. Brain Imaging and Behavior, 10(4), 953–959. https://doi.org/10.1007/s11682-015-9454-9.
Andreassen, C. S., Billieux, J., Griffiths, M. D., Kuss, D. J., Demetrovics, Z., Mazzoni, E., & Pallesen, S. (2016). The relationship between addictive use of social media and video games and symptoms of psychiatric disorders: A large-scale cross-sectional study. Psychology of Addictive Behaviors, 30(2), 252–262. https://doi.org/10.1037/adb0000160.
Arató, Á., Nagy, S. A., Perlaki, G., Orsi, G., Szente, A. T., Kis-Jakab, G., Áfra, E., Alhour, H. A., Kovács, N., Janszky, J., & Darnai, G. (2023). Emotional face expression recognition in problematic Internet use and excessive smartphone use: Task-based fMRI study. Scientific Reports, 13(1). https://doi.org/10.1038/s41598-022-27172-0.
Bachleda, C., & Darhiri, L. (2018). Internet Addiction and Mental and Physical Fatigue. The International Technology Management Review, 7(1), 25–33. https://doi.org/10.2991/itmr.7.1.3.
Brand, M., Young, K. S., Laier, C., Wölfling, K., & Potenza, M. N. (2016). Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: An Interaction of Person-Affect-Cognition-Execution (I-PACE) model. Neuroscience and Biobehavioral Reviews, 71, 252–266. https://doi.org/10.1016/j.neubiorev.2016.08.033.
Caplan, S. E. (2010). Theory and measurement of generalized problematic Internet use: A two-step approach. Computers in Human Behavior, 26(5), 1089–1097. https://doi.org/10.1016/j.chb.2010.03.012.
Darnai, G., Perlaki, G., Zsidó, A. N., Inhóf, O., Orsi, G., Horváth, R., Nagy, S. A., Lábadi, B., Tényi, D., Kovács, N., Dóczi, T., Demetrovics, Z., & Janszky, J. (2019). Internet addiction and functional brain networks: task-related fMRI study. Scientific Reports, 9, 15777. https://doi.org/10.1038/s41598-019-52296-1.
Darnai, G., Perlaki, G., Orsi, G., Arató, Á., Szente, A., Horváth, R., Áfra, E., Nagy, S. A., Kovács, N., Dóczi, T., & Janszky, J. (2022). Language processing in Internet use disorder: Task-based fMRI study. Plos One, 17(6), e0269979. https://doi.org/10.1371/journal.pone.0269979.
Demetrovics, Z., Szeredi, B., & Rózsa, S. (2008). The three-factor model of Internet addiction: The development of the Problematic Internet Use Questionnaire. Behavior Research Methods, 40(2), 563–574. https://doi.org/10.3758/BRM.40.2.563.
Dong, G., DeVito, E. E., Du, X., & Cui, Z. (2012). Impaired inhibitory control in “internet addiction disorder”: A functional magnetic resonance imaging study. Psychiatry Research: Neuroimaging, 203(2–3), 153–158. https://doi.org/10.1016/j.pscychresns.2012.02.001.
Fuchs, M., Riedl, D., Bock, A., Rumpold, G., & Sevecke, K. (2018). Pathological Internet Use—An Important Comorbidity in Child and Adolescent Psychiatry: Prevalence and Correlation Patterns in a Naturalistic Sample of Adolescent Inpatients. BioMed Research International, 2018. https://doi.org/10.1155/2018/1629147.
Gámez-Guadix, M., Calvete, E., Orue, I., & Las Hayas, C. (2015). Problematic Internet use and problematic alcohol use from the cognitive-behavioral model: A longitudinal study among adolescents. Addictive Behaviors, 40, 109–114. https://doi.org/10.1016/j.addbeh.2014.09.009.
Griffiths, M. D. (2014). Internet Addiction Disorder and Internet Gaming Disorder Are Not the Same. Journal of Addiction Research & Therapy, 05(04). https://doi.org/10.4172/2155-6105.1000e124.
Hou, Y., Xiong, D., Jiang, T., Song, L., & Wang, Q. (2019). Social media addiction: Its impact, mediation, and intervention. Cyberpsychology, 13(1). https://doi.org/10.5817/CP2019-1-4.
Hull, M., & Proulx, D. A. (2022). Internet addiction facts and statistics. Umatilla, FL: The Recovery Village.
Lin, L. Y., Sidani, J. E., Shensa, A., Radovic, A., Miller, E., Colditz, J. B., Hoffman, B. L., Giles, L. M., & Primack, B. A. (2016). Association between Social Media Use and Depression among U.S. Young Adults. Depression and Anxiety, 33(4), 323–331. https://doi.org/10.1002/da.22466.
Lin, S. C., Tsai, K. W., Chen, M. W., & Koo, M. (2013). Association between fatigue and Internet addiction in female hospital nurses. Journal of Advanced Nursing, 69(2), 374–383. https://doi.org/10.1111/j.1365-2648.2012.06016.x.
Malik, S., & Khan, M. (2015). Impact of facebook addiction on narcissistic behavior and Self-Esteem among students. Journal of the Pakistan Medical Association. https://www.researchgate.net/publication/275716907.
Mihajlov, M., & Vejmelka, L. (2017). Internet addiction: A review of the first twenty years. Psychiatria Danubina, 29(3), 260–272.
Nachreiner, F. (2001). Time on Task Effects on Safety. Journal of Human Ergology, 30(1-2), 97–102.
Panova, T., & Carbonell, X. (2018). Is smartphone addiction really an addiction? Journal of Behavioral Addictions, 7(2), 252–259. https://doi.org/10.1556/2006.7.2018.49.
Park, S., Kang, M., & Kim, E. (2014). Social relationship on problematic Internet use (PIU) among adolescents in South Korea: A moderated mediation model of self-esteem and self-control. Computers in Human Behavior, 38, 349–357. https://doi.org/10.1016/j.chb.2014.06.005.
Weinstein, A. (2022). Problematic Internet usage: Brain imaging findings. Current Opinion in Behavioral Sciences, 47. https://doi.org/10.1016/j.cobeha.2022.101209.
Williamson, A., Lombardi, D. A., Folkard, S., Stutts, J., Courtney, T. K., & Connor, J. L. (2011). The link between fatigue and safety. Accident Analysis and Prevention, 43(2), 498–515. https://doi.org/10.1016/j.aap.2009.11.011.
Young, K. S. (1998). Internet Addiction: The Emergence of a New Clinical Disorder. Cyberpsychology and Behavior, 1(3), 237–244. https://doi.org/10.1089/cpb.1998.1.237.
Zeller, R., Williamson, A., & Friswell, R. (2020). The effect of sleep-need and time-on-task on driver fatigue. Transportation Research Part F: Traffic Psychology and Behaviour, 74, 15–29. https://doi.org/10.1016/j.trf.2020.08.001.